Life – Terror. Ecstasy. Fight. Denial. Flight. Failure. PAIN. Forgiveness. Reconciliation. Hope. Love. Peace – Death.
The prostate, a walnut-sized gland, sits just below the bladder and has a vital role in male anatomy as it helps make part of the ‘seminal fluid’ and can affect the flow of urine. Prostate cancer is the most common cancer in UK men. It often grows slowly with no early symptoms. Like most cancers, curability, is highest when diagnosed early. Diagnosis is typically, by (PSA) blood test often followed by physical examination if blood testing demonstrates above normal levels of a prostate specific antigen (a protein) produced by the prostate gland.
I was diagnosed with prostate cancer 10 years ago aged 56. In 2015 56 was considered ‘young’ for an advanced prostate cancer diagnosis. 2026, 10 years on, men are contracting prostate cancer much younger. Shockingly, as young as in their teens! It is, so far, inconclusive as to why prostate cancer is evolving from an ‘old man’ disease to an ‘any man’ disease. I was diagnosed by sheer coincidence.
My niece had been receiving treatment for, early age, (non cancerous) bowel polyps. Her medical team had advised “All close relatives” should be screened. I passed my GP these instructions and he advised, “while we are at it we might as well have a prostate check, a PSA test”. I had zero symptoms other than sometimes having to take a piss during the night which I wrote off as age associated.
In recent times we have seen intense campaigning involving charities, Olympian Sir Chris Hoy, who has terminal prostate cancer, as well as former Prime Ministers David Cameron and Rishi Sunak. Many famous faces including actor Stephen Fry and footballer Les Ferdinand have been vocal on an issue that affects many men.
Prostate cancer is the most common cancer in men and kills 12,000 people across the UK each year. Currently, 1 in 4 men will contract prostate cancer in their lifetime. In recent times, there has been mounting pressure to introduce mandatory prostate cancer screening for ALL men of a certain age, similar to breast cancer screening for women. The UK’s National Screening Committee have conducted a study and published a response of their findings with recommendations.
Only “a few thousand” men who have a dangerous genetic variant and a family history of cancer should be screened for prostate cancer with a (PSA) blood test, according to the final recommendations of scientific advisers. The UK’s National Screening Committee says the “harms of screening” outweigh the benefits in all other groups. They suggest that testing “healthy men” for prostate cancer does save lives, but also “leads to treatment that can leave men unable to control their bladder or have an erection”.
This, somewhat sweeping, misleading, statement is not helpful.
A Prostate-Specific Antigen (PSA) test is a simple blood test that measures the amount of PSA (an exclusive to the prostate protein produced by the prostate gland) in your blood. It is primarily used to help diagnose and monitor prostate conditions like prostate cancer, an enlarged prostate (BPH), or prostatitis.
A raised ‘above normal’ PSA test result would initiate further testing, usually a physical examination (by a GP) of the gland, potentially leading to a follow up MRI and if necessary a biopsy. Not necessarily, life-changing treatment such as surgery to remove the gland. The final decision to introduce mandatory prostate cancer screening rests with health ministers in England, Wales, Scotland and Northern Ireland.
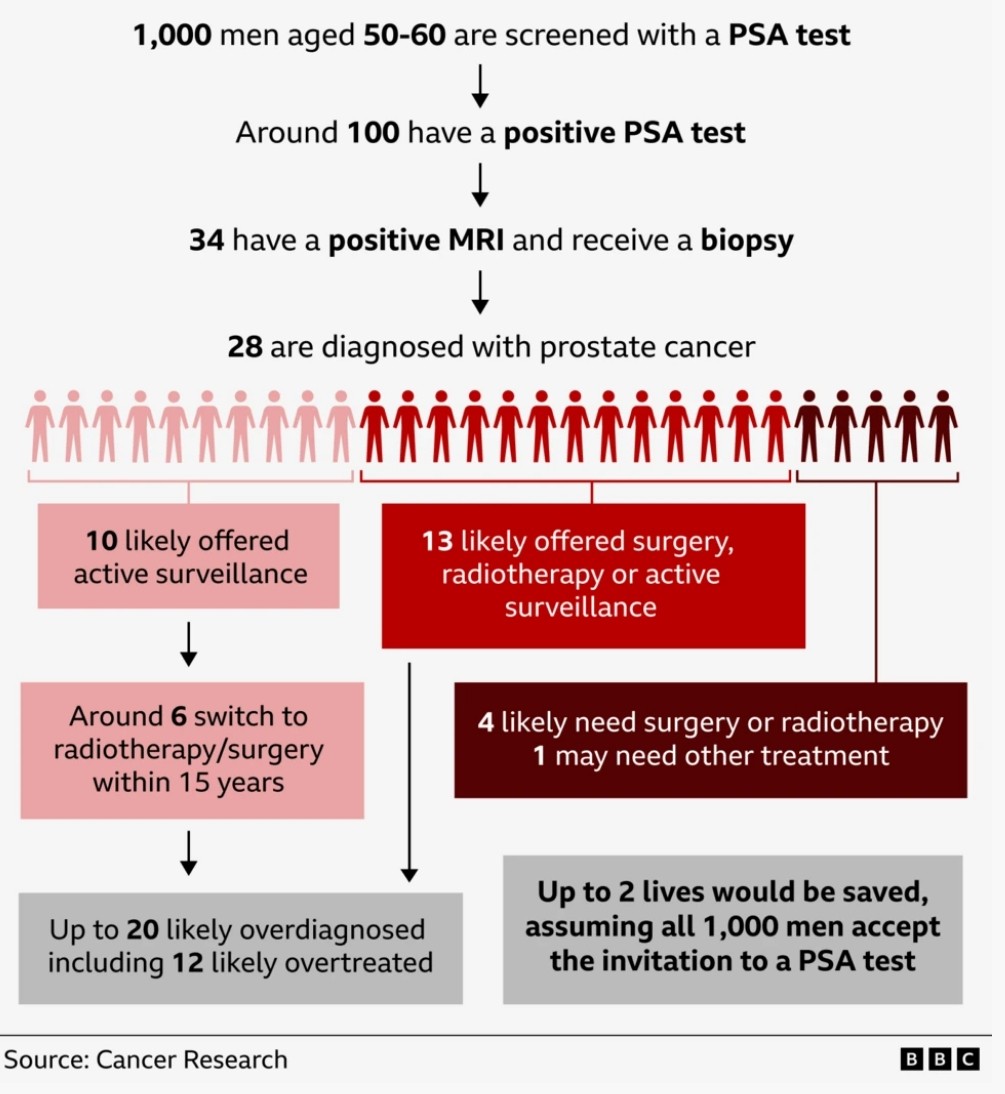
A major review by the National Screening Committee said for every 1,000 men screened in their 50s, it would save two lives from prostate cancer over the next 15 years. But it would also lead to 20 men being told they have a cancer who would never require “active” treatment.
Some prostate cancers grow so slowly you would have to reach 120 to 150 years old before they were a threat. However, they would have to live with that psychological burden of a cancer diagnosis for the rest of their lives.
Out of those 20 men, 12 would end up having treatment they don’t need, but that damages the prostate – potentially damaging their sex lives and causing some incontinence, meaning they would need a pad to catch leaking urine.
“Once a prostate cancer is found, we still can’t reliably tell which cancers need treatment or which do not – and the treatments available for prostate cancer can cause long-lasting harm,” said Prof Sir Mike Richards, who chairs the screening committee and has prostate cancer himself.
The final advice says screening should not be offered to:
- All men
- Black men, who are at double the risk of prostate cancer
- Men with a family history of cancer – as the disease is so common that it doesn’t narrow down the risk
The only group where the benefits were greater than the harms is men with a BRCA2 gene variant and a family history of breast, ovarian, pancreatic, or prostate cancer.
BRCA2 is involved in repairing DNA and some mutations lead to cancers being both more common and more deadly. The screening committee said eligible men should be invited for a PSA blood test every two years between the ages of 45 and 61. This will apply to a “few thousand” men a year, some are already getting informal screening as their families are known to NHS genetics clinics.
The committee (UK NSC) said it would continuously evaluate new evidence as it comes in, which could yet lead to wider screening programmes. This includes new tests for prostate cancer that may do a better job of spotting those that need treatment, (AI) artificial intelligence tools and the results of the Transform trial which is underway in the UK and should soon answer a key area of uncertainty for black men. While it is clear that black men are at much higher risk of getting prostate cancer, it is still uncertain whether those cancers are more dangerous – which would affect the decision on whether the NHS should offer screening. Sir Mike said he hoped “new evidence and new tests and a better understanding of prostate cancer will support wider prostate cancer screening in future” but they “do need the evidence first”.
The final advice suggests screening for even fewer people than was originally suggested in November when people with both BRCA1 and BRCA2 mutations would have been eligible.
Chiara De Biase, from Prostate Cancer UK, said she was “deeply disappointed” with the final recommendations. “We know that a mass screening programme could save thousands of men’s lives, and while we recognise the current evidence does not yet show that screening all men at risk would do more good than harm, today’s decision is a step backwards, narrowing the recommendation to a smaller pool of eligible men.”
What actually changes with prostate screening will be decided by ministers in the devolved governments in the UK. Sir Mike is due to discuss their recommendations with the new health secretary James Murray on Monday [1/06/2026].
Dr Ian Walker, executive director of policy at Cancer Research UK, said: “Screening decisions must be guided by the current evidence”, with programmes only introduced when the benefits are shown to outweigh the harms, including unnecessary and invasive overtreatment. “We urge the UK Government to accept the recommendation.”
This issue was discussed at my recent Prostate Cancer Support Group meeting (with patients and clinicians present). I was alarmed to discover that ‘some’ GP’s are reluctant, even refusing to sanction PSA tests. Why? The consensus was that it was not just the test in isolation but it was what the test might lead to? Further expensive testing, treatments, life long care? GP’s no longer see this as sustainable to facilitate? A lengthy (financial)? Commitment. “Overdiagnosis”: The test detects slow-growing tumours that would never cause harm or symptoms during a man’s lifetime. “Watchful Waiting”: in many cases is a far more, long term, economical (efficient)? Treatment strategy?
The Bottom Line
The UK (NHS): The UK National Screening Committee (UK NSC) officially advises against mass screening for all men. However, they recommend targeted screening every two years for men aged 45 to 61 who carry a pathogenic BRCA2 gene mutation and have a relevant family history of cancer.
If you are diagnosed early enough there is a realistic chance of cure. I was diagnosed, by chance, unfortunately, too late, no cure. Post diagnosis I paid for private DNA Testing to establish if I had BRCA1 and BRCA2 mutations as that might effect my son and 4 grandsons. I did not have the genetic mutations. Two things, 1. utter relief, that it is highly unlikely that my DNA could effect my son and grandsons chances of contracting Prostate Cancer. 2. If I had not had a “random” PSA test I would not have known I had prostate cancer and would, most likely, now, be dead.
Advice
Every male over 30 should have, recurring, PSA testing, at least every 12 months. If you have never had a PSA test, have one, now, today!
To get an NHS PSA test in Liverpool, you should contact your registered GP, as they do not currently offer broad population-level screening in the UK. If you are over 50 or experiencing symptoms and wish to be tested, UK guidelines state you are entitled to one after discussing the implications with your doctor. You might need to be a bit economical with the truth, “Dr, I have been getting up 2 or more times during the night to pee? My pee is taking longer….after peeing I still feel there is more? It is slightly painful to pee nowadays”?
There are numerous private (paid for) PSA testing services available (do a simple online search). However, U-Test Prostate PSA at-home self-testing kits are available across all Home Bargains stores. These rapid finger-prick blood tests are MHRA-registered and are designed to measure Prostate-Specific Antigen (PSA) levels, providing visual results on a test cassette within 3 to 10 minutes for as little as a bar of chocolate (£2.99). DNA testing, to establish the presence of BRCA2 gene mutation, is much more expensive and not currently available via the NHS.
NHS GP PSA TEST – Preparing for the Test
To ensure your PSA reading is accurate, you must avoid the following in the 48 hours prior to your blood test:
- Ejaculation or sexual activity
- Vigorous exercise (such as cycling)
- Having any active urinary tract infection (UTI) within the last 6 weeks
Understanding Your Results
PSA levels are measured in nanograms per millilitre of blood (\(ng/mL\)). While most men have a PSA level lower than \(3 ng/mL\), there is no single “normal” number. Target levels can rise naturally as you age and depending on the size of your prostate.
A high or rising PSA level does not automatically mean you have cancer. Levels can also be elevated due to:
- An enlarged prostate
- Prostatitis (inflammation or infection of the prostate gland)
- Urinary tract infections (UTIs)
Because a PSA test cannot distinguish between cancerous and non-cancerous changes, it serves as a first-line investigation. If your levels are raised, you can initiate an informed conversation with your GP. Your GP may recommend further investigations, such as a physical examination, MRI scan, or biopsy. For comprehensive and balanced information on the benefits and risks of having the test, you can review the Prostate Cancer UK PSA Blood Test Guide.
Expert Recommendation
Leading charities like Prostate Cancer UK strongly advise that anyone worried about prostate cancer bypass rapid self-tests and instead consult a GP for a reliable, professional blood test and proper clinical evaluation.
My initial, self initiated, PSA result (2015) was 13. After a rectal examination my GP informed me there and then, “you probably have cancer” and referred me for a urology consultation leading to a treatment plan. I am 10 years alive.
Get tested dudes!
Thanks for Reading
#Peace
